
Every year, over 1.5 million people in the U.S. are harmed by mistakes in their prescriptions. Many of these errors happen before the pill even leaves the doctor’s office. You might think your doctor or pharmacist has it covered-but the truth is, prescription writing errors are more common than you realize, and you’re the last line of defense. A wrong dose, a confusing abbreviation, or a mix-up between two similar-sounding drugs can lead to serious harm-or even death. The good news? You don’t have to wait for something to go wrong. With a few simple checks, you can catch these mistakes before they hurt you.
What Are Prescription Writing Errors?
Prescription writing errors are mistakes made by doctors or other providers when they write or enter a medication order. These aren’t pharmacy mistakes-they happen at the source. They can be as simple as a sloppy handwriting, or as dangerous as writing ‘U’ for units instead of spelling out ‘units.’ That tiny error can turn a 5-unit insulin dose into 50 units, which could send someone into a life-threatening low-blood-sugar coma. According to the Institute of Medicine, these kinds of errors cause at least 1.5 million injuries every year. The most common types include:- Wrong dosage or quantity (19% of all errors)
- Illegible handwriting (22% of errors)
- Incorrect frequency instructions (like ‘QD’ instead of ‘once daily’)
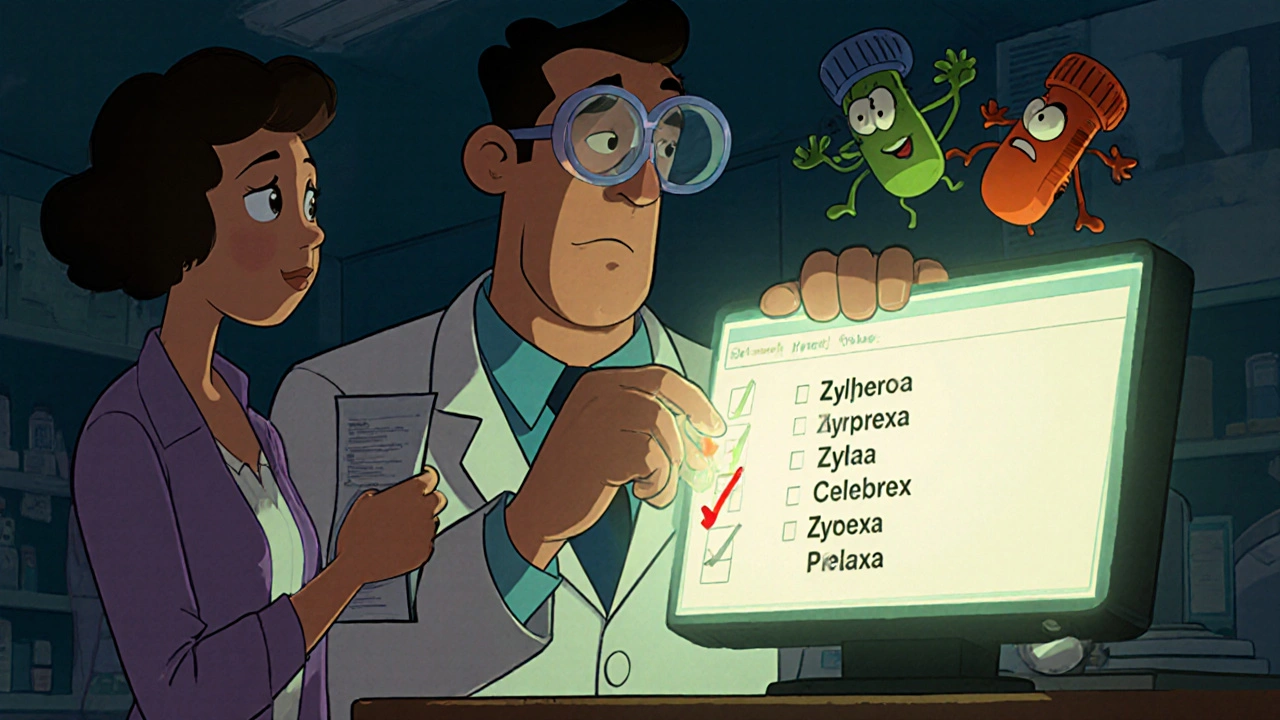
- Drug name mix-ups (like Celebrex vs. Celexa)
- Missing or unclear purpose for the medication
- Use of dangerous abbreviations like ‘MS’ for morphine sulfate (which can be confused with magnesium sulfate)
High-Risk Medications You Need to Double-Check
Not all medications carry the same risk. Some are called “high-alert” because even a small mistake can be deadly. These include:- Insulin
- Warfarin (blood thinner)
- Hydrocodone and other opioids
- IV potassium chloride
- Heperin (anticoagulant)
The Seven-Point Prescription Checklist
The FDA and patient safety experts agree: if you check these seven things every time you get a prescription, you’ll catch most errors before they reach your medicine cabinet.- Full drug name-No abbreviations. ‘Lamictal’ is a brand name. The generic is ‘lamotrigine.’ If it’s written as ‘Lamictal’ without the generic, ask why. Brand names can be confused with other drugs.
- Precise dosage-It should use leading zeros (0.5 mg, not .5 mg) and avoid trailing zeros (5 mg, not 5.0 mg). Trailing zeros can make a 5 mg dose look like 50 mg.
- Clear frequency-Avoid ‘QD,’ ‘BID,’ ‘TID,’ or ‘QID.’ These are outdated abbreviations. It should say ‘once daily,’ ‘twice daily,’ etc.
- Total quantity-If you’re told you’ll take it for 10 days, does the prescription say 10 pills-or 100? A typo here can mean you run out early-or have too much.
- Purpose of the medication-It should say why you’re taking it: ‘for high blood pressure,’ ‘for anxiety,’ etc. If it’s blank, ask. This helps catch wrong prescriptions.
- Prescriber’s contact info-If the phone number or signature is missing, the pharmacy can’t call to verify. That’s a red flag.
- Expiration date-Prescriptions expire. If it’s more than a year old, ask if it’s still valid.
Red Flags to Watch For
Some mistakes are easy to spot if you know what to look for:- ‘U’ for units-Always spelled out as ‘units.’
- ‘MS’ or ‘MSO4’-Could mean morphine sulfate or magnesium sulfate. These are completely different drugs. One calms pain. The other stops heart rhythms.
- ‘HC’ for hydrocortisone-Can be mistaken for heparin, a blood thinner. A mix-up here can cause bleeding.
- ‘ug’ for micrograms-Often confused with ‘units.’ Insulin errors from this mistake have killed people.
- Look-alike/sound-alike drugs-Zyprexa (antipsychotic) vs. Zyrtec (allergy pill). Celexa (antidepressant) vs. Celebrex (arthritis drug). These pairs are on the ISMP’s official error-prone list.
Use the Teach-Back Method
Don’t just nod and walk out. After your doctor explains your prescription, repeat it back in your own words. This is called the teach-back method-and it works. Say something like: ‘So, I take one 5 mg tablet of lisinopril once a day for my blood pressure, right?’ Johns Hopkins Medicine found this simple step reduces misunderstandings by 81%. It forces the provider to clarify if they made a mistake. And if they’re annoyed? That’s a red flag too. Good providers welcome questions.Verify Electronic Prescriptions
Even if your doctor sends the prescription electronically, mistakes still happen. Pharmacies get the wrong drug because the system auto-filled ‘amoxicillin’ instead of ‘azithromycin.’ When you pick up your prescription, compare the label to your checklist. Does the name match? The dose? The frequency? If it doesn’t match what your doctor told you, don’t take it. Ask the pharmacist to call the doctor. New tools can help. Apps like MedSafety let you take a photo of your prescription and scan it for errors. In a 2023 pilot study, users caught 68% more mistakes using the app.Ask the Right Questions
The National Patient Safety Foundation’s ‘Ask Me 3’ program gives you three simple questions to ask every time you get a new medication:- What is my main problem?-This confirms the diagnosis matches the drug.
- What do I need to do?-Clarifies the dose, timing, and duration.
- Why is it important for me to do this?-Helps you understand the risk of skipping it or taking it wrong.





Erika Sta. Maria
Okay but have you ever seen a doctor’s handwriting? I once got a script that looked like a toddler’s abstract art. The pharmacist spent 20 minutes calling the office. Turns out it was ‘amoxicillin’-but it looked like ‘amoxicilin’ with a spiral and a doodle of a dinosaur. I swear, we’re one typo away from a national crisis. 🤯
Elaina Cronin
It is imperative to underscore the gravity of this issue. The systemic failure of medical documentation protocols constitutes a gross dereliction of duty on the part of healthcare institutions. The onus of patient safety should not rest upon the shoulders of the layperson. This is not a checklist-it is a indictment of a broken system.
Willie Doherty
Statistically, 63% error detection via patient checklist is a misleading metric. The sample size of the University of Michigan study was n=127, with 43% of participants being medical students. Also, ‘teach-back method’ has a 27% failure rate in non-native English speakers. You’re advocating for a solution that assumes cognitive literacy and linguistic privilege. That’s not safety. That’s gatekeeping.
Darragh McNulty
Y’all are overcomplicating this 😊 Just ask three simple questions: What’s this for? How much? When? 🙌 Your life is worth it. And if your doc gets mad? That’s their problem. You’re not being annoying-you’re being alive. 💪
Cooper Long
The notion that patients must act as medical auditors reflects a profound erosion of professional accountability. The responsibility for accurate prescribing lies with licensed practitioners, not with individuals lacking clinical training. This article, while well-intentioned, normalizes a dangerous shift in liability.
Sheldon Bazinga
lol why are we even talking about this like its a big deal? doctors are just tired af. i got a script for 100mg of zoloft once and the doc wrote 10mg. i took it anyway. felt like a zombie for 3 days. whatever. we all know the system is trash. just dont take pills you dont understand. 🤷♂️
Sandi Moon
Let’s be honest-this is all part of the Great Pharma Agenda. The ‘seven-point checklist’? A distraction. The real issue is that EHR systems are owned by private corporations that profit from error escalation. The ‘MS’ confusion? Deliberate. The ‘U’ for units? Designed to cause chaos so they can sell you more ‘safety apps.’ Blockchain? Just a new way to track your meds and sell your data. You’re being played. Always have been.
Kartik Singhal
Look, I’m Indian. We’ve been doing ‘medication yoga’ since birth. Grandma would stare at the bottle for 10 minutes before swallowing. ‘Is this for my liver or my soul?’ 😏 The checklist? Cute. But real safety? It’s in the silence before you swallow. The pause. The doubt. The unspoken question: ‘Why am I still alive after this?’ 🧘♂️💊
Logan Romine
So let me get this straight… we’ve got AI that can write sonnets and predict your crush’s birthday, but we still can’t get a computer to spell ‘milligrams’ without a decimal typo? 🤡
And the FDA’s gonna add ‘pictograms’? Next they’ll put a little stick figure of a man taking a pill next to ‘ibuprofen.’
Meanwhile, I’m over here Googling ‘is this pill a dinosaur?’
At this point, I just hold the bottle up to the sun and whisper, ‘Are you trying to kill me?’
…and then I take it anyway. 😌